How to Use Neuroscience to Stop Hiccuping. Immediately.

Are you hiccuping right now? Stop whatever you’re doing, and follow these instructions to the letter. I promise it'll probably help.
- Fully exhale, removing all the air from your lungs.
- Breathe in deeply and hold it in for ten seconds.
- Without breathing out, inhale once more, and hold that for five more seconds.
- One last time, without exhaling, breathe in again, hold for five.
- Exhale.
Your hiccups should be gone. If they aren’t, try these other methods:
- Sitting or lying down, take a deep breath, then for fifteen seconds, push that breath out against your closed nose and mouth. Exhale after.
- Swallow a spoonful of sugar.
- Sip cold water.
- Hold crushed ice in your mouth.
If none of these solutions are working, it’s alright to just wait your hiccups out. Most cases of singultus (the medical term for hiccups) go away after a couple minutes. But just like with Viagra, seek out a doctor if it lasts four hours or more. I'm willing to bet that at least one of these methods has resolved your issue. Why did it work, though?
Now that I've covered the information that you may immediately require (this isn't a cooking blog; you won't get my whole life story before the recipe), let's discuss:
- What hiccups actually are
- Why we hiccup
- How the methods I listed above utilize our knowledge of human neurobiology to put an end to those irritating diaphragmatic spasms
- The oddities of hiccup history (hiccupstory?)
This article is quite comprehensive, so I've organized it into sections. Feel free to scroll to the headers of the topics that interest you most.
What Is a Hiccup?
A hiccup is a coordinated series of involuntary contractions by:
- The diaphragm, the muscle that inflates and deflates your lungs
- The intercostal muscles, which expand and contract your chest cavity during heavier breathing
- Your glottis, the upper entrance to your vocal cords
During singultus, you inhale rapidly and forcefully, snapping your glottis shut and shoving air into it. That's what produces that signature "hic" sound. You can even hiccup manually if you want — try it! Take a deep, rapid breath and close off your airway almost immediately after you start breathing in, getting ever so slightly vocal with it.
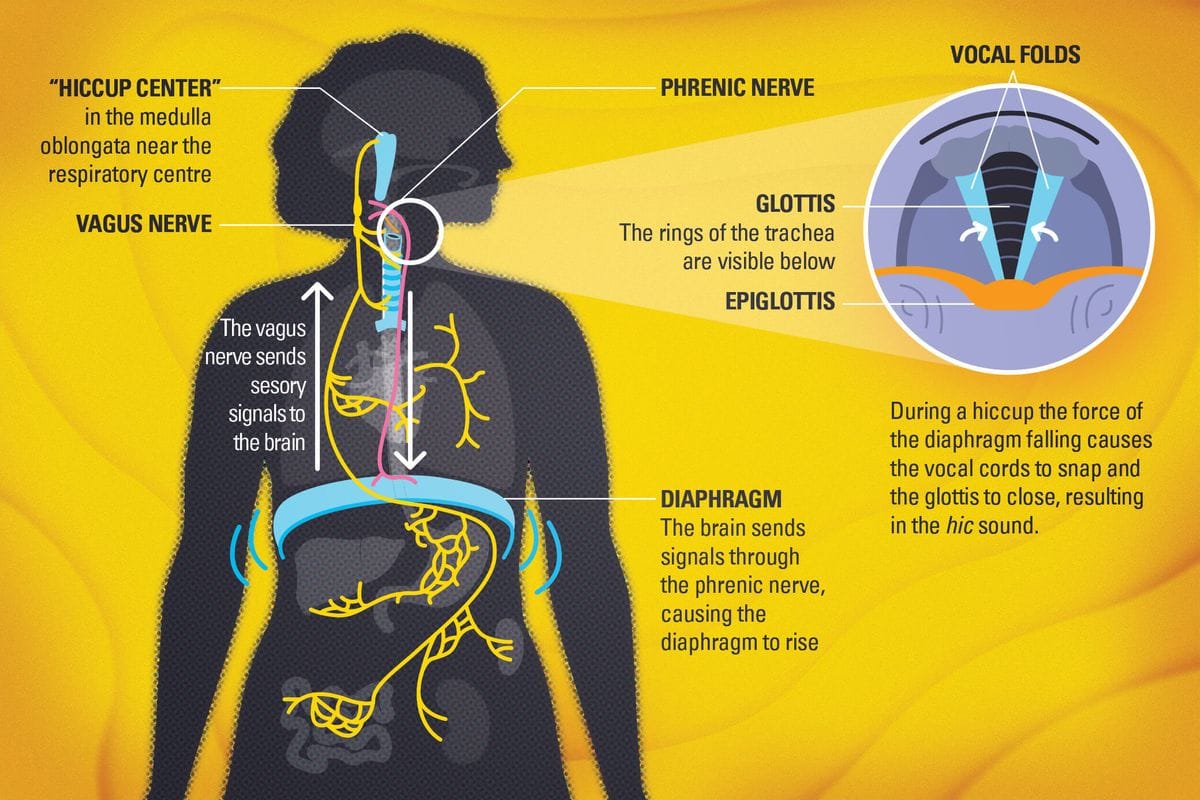
Neurologically, hiccuping is believed to originate from a group of brain cells, known together as the hiccup central pattern generator, or CPG, for short. The CPG lies within the brain stem, specifically within the medulla. This general area is known as the "lizard brain," because it controls important primitive functions like breathing, heart rate, and basking on rocks under the sun. Like a vegan who never shuts up about their (admittedly morally correct) lifestyle, the CPG constantly attempts to send out hiccup commands to your respiratory muscles on a repeating timer. Your brain permanently blocks these signals from reaching your body, but whenever this inhibitory mechanism fails, you start hiccuping to the beat of the CPG's drum.
Why Do We Hiccup?
It's not actually clear why we hiccup. The only academic consensus we've reached is that for adult humans, hiccuping is almost certainly useless. It's not actively harmful, unless it lasts for years on end (don't worry, we'll get to that), but it doesn't appear to serve any function whatsoever. However, there are several theories on the origin of hiccuping, and they all trace back to our pasts, both within and outside our own lifetimes.
Our brain stems might not know that we aren't frogs

Tadpoles, the larval stage of amphibians like frogs and salamanders, reach a period during their development where their bodies have both functioning gills and functioning lungs, enabling them to swap between breathing air and water at will. For these tadpoles, breathing either source of oxygen works basically the same way. For water: take a big sip, close off the entrance to your windpipe, and sharply inhale to force the contents of your mouth down your esophagus and across your gills. Breathing air is more or less the same, except you close off your esophagus instead of your windpipe and force air into your lungs instead of down your throat.
If this sounds familiar, that's because it is. Tadpoles in their multimodal stage breathe exclusively by hiccuping, regardless of if they're breathing air or water. The only difference is that, as adolescent amphibians, they always have a pipe for the fluid to travel down, ensuring that every hiccup results in a breath. This respiratory action is mediated by a group of neurons in the tadpole's brain stem that sends out coordinated signals on a repeating timer – a CPG, likely a close match to the original version of our own.
The implication taken from this perspective is that when we stopped being amphibians and started being animals that only breathe air, we developed additional neural circuitry for controlling lungs and diaphragms, but instead of removing our primitive tadpole breath circuit, we simply stuck a large sign onto it that reads, "DO NOT USE," and assigned an occasionally-inattentive guard to prevent us from hiccuping.
In essence: if our brain doesn't constantly dedicate time to reminding itself that it isn't a frog, it will start to breathe like one.
Hiccuping might be an anti-baby-death device

Babies are notoriously bad at staying alive. Sudden Infant Death Syndrome is an entire condition dedicated to diagnostically saying, "yeah, they just do that sometimes." It stands to reason that any babies with beneficial traits helping them stay alive during their earliest, most vulnerable developmental period are more likely to live long enough to pass on those traits to their progeny. There is evidence to suggest that hiccuping is one of these traits – that hiccuping serves a vital purpose in protecting infants from harm, and that the occasional bouts of singultus we experience later in life are a byproduct of being alive long enough to complain about them.
Nursing infants swallow a lot of air alongside the milk they consume, and this acts as a limiting factor for how much a baby can drink, as the air takes up important space in their stomach that could otherwise be used to store and digest nutrients. Interestingly, hiccuping creates a strong pressure vacuum in an infant's upper respiratory system, facilitating the extraction of gas out from the stomach and up into the esophagus, perfectly positioned to be expelled by a burp. Hiccuping promotes burping, which promotes higher nutrient consumption, which promotes health and growth, which increases the odds of surviving to adulthood.
If you want your child to grow big and strong, make sure they drink plenty of milk, hiccup constantly, and burp as much as possible. You can always teach them to say "excuse me" later.
Why Are These Treatment Methods Effective?
At the beginning of this article, I listed several techniques to quickly and effectively treat singultus. While there is no guaranteed cure-all, these are the methods that exploit the way our brain and body works and that have been shown to succeed most often. Let's quickly go through them one-by-one, just to explain how and why each treatment is intended to stifle the hiccups.
- Supra-supramaximal Inspiration (SSMI): This is the first thing I recommended trying at the very top of the article. Breath-holding is one of the oldest and most well-known hiccup remedies, and that's probably because it actually works. Holding your breath builds up carbon dioxide in your bloodstream, which relaxes both your diaphragm and your nervous system, reducing the likelihood of any errant spasms due to neurological excitability. Research suggests that it also forces the parts of your brain that govern breathing to focus, shifting increased attention back towards inhibiting the hiccup CPG. SSMI is simply optimized breath-holding for getting rid of the hiccups.
- The Valsalva Maneuver: The second recommended approach, this is basically holding your breath and trying to pop your ears like you're on a turbulent airplane ride. Aside from what SSMI already does, this maneuver aims to overwhelm and briefly overload and interrupt the vagus nerve, the primary transport vessel for the hiccup CPG's signaling. Temporarily cordoning off the path from the brain stem to the rest of the body provides an additional opportunity to re-stabilize. Exercise caution performing this maneuver, though – unlike with SSMI, you're not often inhaling here, so you might pass out if you try this method for half an hour straight. On the bright side, it's quite difficult to hiccup while unconscious.
- Sipping cold water, holding crushed ice in your mouth, and swallowing spoonfuls of granulated sugar all conform to the same idea: if you can overwhelm the vagus nerve with enough simultaneous or intense input, it will only focus on standard breathing and won't have the bandwidth for transmitting hiccup signals. The temperature shock of ice and cold water, the granularity of every individual particle of sugar hitting your throat (like your hiccups are a vampire that has to stop and count every grain before continuing to terrorize you), and even the vestibular confusion induced by the Valsalva maneuver all follow this principle. In fact, if there's any other strange folk remedy for hiccups that you swear by, it probably does too.

The Oddities of Hiccup History
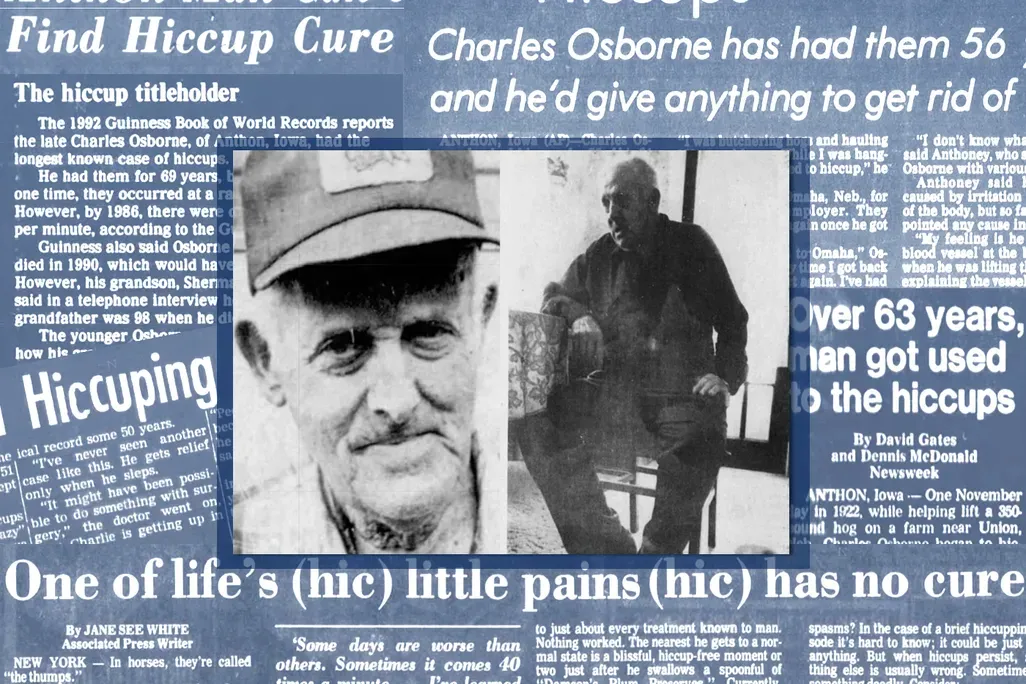
- An Iowa farmer hiccuped more than 430 million times over 68 years after he fell and suffered a brain injury that destroyed the area of the brain stem that acts as the first line of inhibitory defense against the hiccup CPG.
- According to Ancient Greek tradition, having the hiccups indicates that someone's gossiping about you; you can rid yourself of the condition by correctly guessing the identity of the gossiper and speaking their name aloud.
- Antidepressants and pain medications are often prescribed as effective treatments for serious hiccuping; they serve to relax the nervous system, reducing neural excitability and allowing for autonomous control.
- Over the eighties and nineties, several "incurable" cases of hiccups have been resolved via invasive prostate exams; this is still used as a last-ditch effort to cure the hiccups, especially if medical interventions such as medication have proven to be ineffective. Several years later, another case was resolved via the patient achieving orgasm. Upon learning this, the doctor who originally discovered the "rectal method" expressed that his own strategy was inferior in design. In case you're wondering – yes. These are both avenues that stimulate the vagus nerve.
Well, there you have it. That's everything you ever wanted to know about hiccups, and everything you didn't want to know, too. Burp your babies, hold your breath, and keep tabs on your hiccup CPG. If all else fails, look yourself in the mirror and firmly remind yourself: "I am not a frog."
WORKS CONSULTED
Straus C, Vasilakos K, Wilson RJ, Oshima T, Zelter M, Derenne JP, Similowski T, Whitelaw WA. A phylogenetic hypothesis for the origin of hiccough. Bioessays. 2003 Feb;25(2):182-8. doi: 10.1002/bies.10224. PMID: 12539245.
Howes D. Hiccups: a new explanation for the mysterious reflex. Bioessays. 2012 Jun;34(6):451-3. doi: 10.1002/bies.201100194. Epub 2012 Feb 29. PMID: 22377831; PMCID: PMC3504071.
Steger M, Schneemann M, Fox M. Systemic review: the pathogenesis and pharmacological treatment of hiccups. Aliment Pharmacol Ther. 2015 Nov;42(9):1037-50. doi: 10.1111/apt.13374. Epub 2015 Aug 25. PMID: 26307025.
KAHRILAS PJ, SHI GWhy do we hiccup?Gut 1997;41:712-713.
Launois S, Bizec JL, Whitelaw WA, Cabane J, Derenne JP. Hiccup in adults: an overview. Eur Respir J. 1993 Apr;6(4):563-75. PMID: 8491309.
Petroianu GA. (2014). The treatment of hiccup. Expert Opinion on Pharmacotherapy, 15(7), 987–996.
Wang T, Wang D. Metoclopramide for patients with intractable hiccups: a multicentre, randomised, controlled pilot study. Intern Med J. 2014 Dec;44(12a):1205-9. doi: 10.1111/imj.12542. PMID: 25069531.
Zhang C, Zhang R, Zhang S, Xu M, Zhang S. Baclofen for stroke patients with persistent hiccups: a randomized, double-blind, placebo-controlled trial. Trials. 2014 Jul 22;15:295. doi: 10.1186/1745-6215-15-295. PMID: 25052238; PMCID: PMC4223604.
Friedman NL. Hiccups: a treatment review. Pharmacotherapy. 1996 Nov-Dec;16(6):986-95. PMID: 8947969.
Kolodzik PW, Eilers MA. Hiccups (singultus): review and approach to management. Ann Emerg Med. 1991 May;20(5):565-73. doi: 10.1016/s0196-0644(05)81620-8. PMID: 2024799.
National Institute of Neurological Disorders and Stroke. Hiccups Fact Sheet. (NINDS.gov)
American Academy of Neurology (AAN). Guidelines for the management of persistent hiccups (internal resource via case reviews).
Odeh M, Bassan H, Oliven A. Termination of intractable hiccups with digital rectal massage. J Intern Med. 1990 Feb;227(2):145-6. doi: 10.1111/j.1365-2796.1990.tb00134.x. PMID: 2299306.